Thesis
In 2023, studies showed that 33.9% of the US population suffered from anxiety, 24.3% suffered from chronic pain, and 15.9% suffered from some sort of addiction. These conditions have direct and indirect costs for the US economy every year. For example, chronic pain cost $722.8 billion in 2021. In 2023, the US incurred $820 billion in yearly costs as a result of drug abuse. While anxiety’s costs are harder to measure, mental illnesses, including anxiety, were calculated to cost $282 billion a year in 2024. While first-line treatments consisting of drug and behavioral therapy have been adopted, 30-60% of patients are resistant to treatment for anxiety, at least 40% of chronic pain patients “fail to achieve adequate relief”, and 40-60% of patients undergoing treatment relapse.
Meanwhile, the neurotechnology market is projected to grow from roughly $15.3 billion in 2024 to $52.9 billion by 2034 (13.2% CAGR), with sub-segments such as neuromodulation (9.4% CAGR), brain–computer interfaces (16.7% CAGR), and neuro-diagnostics (3.1% CAGR) growing in parallel. 2024 saw $2.3 billion in venture financing for neurotech, compared with $23 billion in funding raised overall by US healthcare companies. This is consistent with early, pre-inflection periods in other long-cycle device and biotech categories, such as cell and gene therapy, where $1.3 billion in venture funding was raised in 2016. In 2018, after the FDA approved its first gene therapies for cancer in August 2077 and inherited disease in December 2017, gene therapy companies raised $2.9 billion, a 133% increase.
Regulatory and payment environments have also become more accommodating to neurotechnology. The FDA’s Breakthrough Devices Program serves to expedite “development, assessment, and review for premarket approval” for neuro-devices. This allows companies to work directly with the FDA in 45-day sprints, as opposed to 60- 75-day waits. The Centers for Medicare & Medicaid Services (CMS) has a Transitional Coverage for Emerging Technologies (TCET) pathway that allows manufacturers to obtain provisional Medicare coverage during evidence generation. Private insurers follow CMS’s example on what they cover and how much they will pay. These shifts reduce the gap between technical validation and commercial access to patients, improving the odds that clinically positive signals translate to paying users.
Technically, non-invasive neuromodulation has crossed important thresholds. Low-intensity focused ultrasound can engage deep brain targets with millimeter-scale focality and can be planned and verified with MRI. This addresses the depth–focality trade-off (increasing stimulation depth while decreasing stimulation focus) faced by surface-level tools, such as Transcranial Magnetic Stimulation (TMS), and has led to invasive implants becoming the primary medical device type for deep-brain clinical problems. At the same time, public sentiment remains reluctant toward invasive BCIs, creating relative openness to non-surgical alternatives; federal R&D programs (e.g., DARPA N3) have further validated national-level interest in non-invasive neural interfaces.
Nudge is a neurotechnology company developing non-invasive, MRI-verified focused-ultrasound systems aimed at modulating deep brain circuits implicated in anxiety, OCD, depression, addiction, and chronic pain. Its lead product is a dual-purpose brain imager and stimulator that uses focused ultrasound with imaging-based targeting to modulate defined circuits and measure associated symptom changes. The platform is initially oriented toward conditions with high unmet need and partial treatment resistance, including anxiety, chronic pain, and addiction. However, its broader vision is “to build a headphone-like version [of its product] that could eventually enhance mood, cognition, and overall mental well-being for healthy individuals.”
Founding Story
Nudge was founded in 2024 in San Francisco by Fred Ehrsam (CEO), Jeremy Barenholtz (President & CTO), and Quintin Frerichs.
Ehrsam graduated from Duke University with a BS in computer science and economics in 2010. He co-founded Coinbase with Brian Armstrong in 2012 and served as President through 2017 before transitioning to the board, helping the company scale from inception to a regulated, security-critical consumer platform. Ehrsam brings operating experience in compliance- and risk-heavy environments, which helps inform Nudge’s approach to building a regulated medical device company.
Barenholtz holds a BS in discrete mathematics and computer science and a master's in computer science from Stanford, which he completed in 2021. From 2021 to 2024, he served as VP of Product & Technology at Neuralink, where he worked on integrating electronics and neural interfaces into implantable brain–computer systems. His background in hardware, firmware, and real-time software under clinical and verification constraints carries over to Nudge’s non-invasive platform, where ultrasound drive electronics, control systems, and MRI-guided targeting must function as a coherent clinical device.
Frerichs studied computer science and philosophy-neuroscience-psychology at Washington University in St. Louis. He developed whole-brain neuroimaging software for Johns Hopkins from 2020 to 2021, then joined the founding team at Arcadia Medicine to work on psychedelic-assisted therapy research for generalized anxiety disorder, major depressive disorder, and substance use disorder; he remains a strategic advisor. His work in imaging tooling and with anxiety/depression/SUD populations shapes Nudge’s emphasis on imaging-driven targeting.
Product
Scientific Foundations
Nudge’s platform is a non-invasive neuromodulation system. Still undergoing clinical studies, it temporarily increases or decreases activity in specific brain circuits and is used to observe how this affects symptoms such as involuntary shaking in movement disorders (e.g., Parkinson’s disease). In this context, neuromodulation refers to altering the activity of specific brain circuits using energy or pharmaceutical agents. Nudge’s platform uses energy in the form of ultrasound waves and is non-invasive: nothing penetrates the skin, no device is implanted, and no opening in the skull is required.
The platform delivers low-intensity focused ultrasound (LIFU) from outside the head to a predetermined brain region. Ultrasound waves can pass through the skull and brain tissue without surgery, and their path and strength can be modeled in advance so that the dose remains within predefined safety limits. The low intensity is intended to minimize tissue damage along the beam path and to reduce the likelihood of unintentionally stimulating other brain regions, with the goal of modulating function without creating lesions.
To concentrate the energy, the system uses several emitters placed at different points around the head. Each emitter sends a low-intensity wave from a different angle. By precisely controlling timing, these waves meet at a small region in the brain, where their energy adds up. This creates a relatively tight focus on the intended structure while keeping the energy lower elsewhere. The focus can be moved electronically by changing the timing of the waves, without physically repositioning the hardware. Because no opening in the skull is required, typical surgical risks such as infection and bleeding are reduced, and patients can return for repeated sessions with adjusted doses and targets if the clinical plan changes.
Before a session, MRI scans map the patient’s brain anatomy and help estimate how the skull will affect ultrasound transmission, informing where and how energy is delivered. During or after a session, follow-up imaging and physiological measurements can be used to verify where the energy was delivered and whether the intended structure was engaged, thereby supporting consistent targeting and monitoring across multiple sessions.
Nudge’s approach sits alongside existing neuromodulation options such as transcranial magnetic stimulation (TMS) and deep brain stimulation (DBS). TMS uses a changing magnetic field outside the head to create brief electrical currents in the brain. It is non-invasive and works best on brain regions near the surface. Reaching deeper structures usually involves a trade-off between depth and precision: the deeper the target, the more surrounding areas are affected, so multiple unintended brain regions may be influenced when TMS is used for deep targets.
DBS uses a more invasive approach. It reaches deep brain structures with high precision using surgically implanted electrodes connected to a device that provides continuous or intermittent stimulation. DBS can be effective for certain conditions but depends on brain surgery, implanted hardware, and ongoing device management and follow-up. Nudge’s LIFU approach focused ultrasound has features in common with both approaches: like TMS, it is non-invasive and delivered from outside the skull; like DBS, it is intended to reach deep targets under MRI guidance, while allowing parameters and targets to be adjusted across sessions as needed.
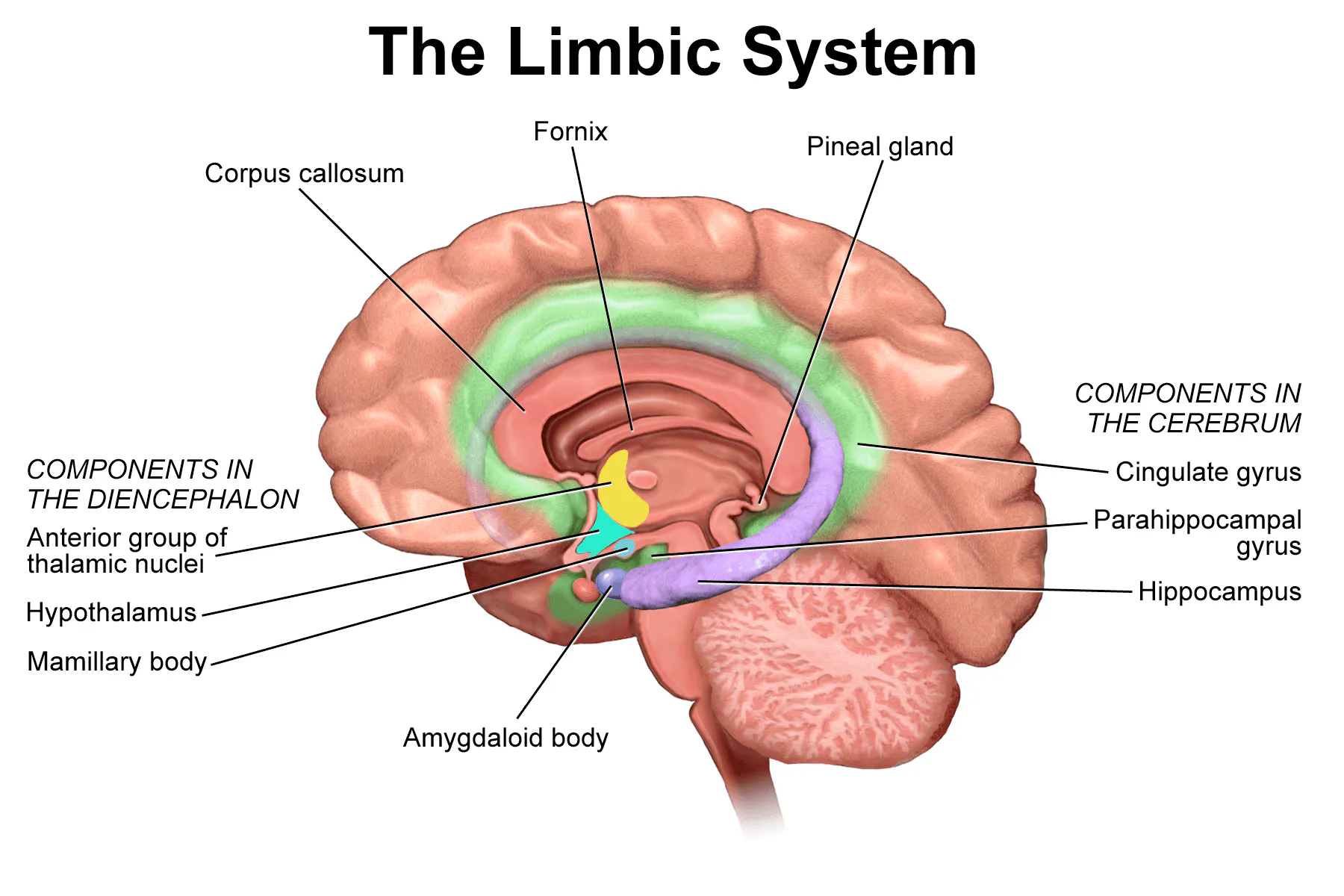
Condition relevance depends on circuit anatomy. For anxiety, limbic (pictured above) and prefrontal networks that control threat detection and arousal include deep and midline nodes that are accessible to focused ultrasound. Pilot studies assess whether reducing excitability at such nodes lowers standardized symptom scales.
Source: Wikipedia
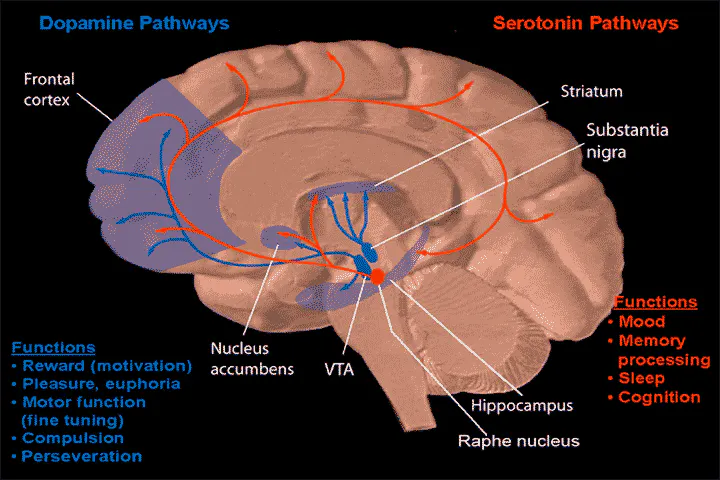
For addiction, the nucleus accumbens and connected frontal circuits (above) support reward valuation and cue reactivity. Non-invasive modulation is being tested against craving measures and task-based biomarkers.
Source: Wikipedia
For chronic pain, thalamic and cingulo-frontal systems mediate sensory and affective dimensions. Early work examines whether targeted ultrasound changes pain ratings and associated physiological measures.
The evidence base comprises animal studies and small-scale human feasibility trials that report measurable changes in neural activity and short-term behavior within accepted ultrasound safety limits. Larger controlled studies with standardized dosing, longer follow-up, and device-class safety monitoring are still needed to determine effect sizes, durability, and generalizability across sites.
Nudge Zero

Source: Nudge
Nudge Zero is a helmet-like device that sits on a patient’s head while they are inside an MRI scanner. It utilizes multiple small ultrasound emitters that are synchronized to produce sound waves that converge at a predetermined point within the brain. The aim is to reach deep structures without the need for surgery or implants. According to Nudge, an initial version was built in roughly six months and then iterated upon. The intended setting is hospitals and research centers rather than everyday or take-home use.
MRI is used to plan where to aim, to guide sessions, and to assess what was achieved. Structural MRI helps select targets and estimate how sound moves through the skull. Nudge also reports an MR-based acoustic radiation force imaging method to visualize where the ultrasound energy actually lands. That readout supports per-patient mapping of stimulation sites and responses. The current design prioritizes wide brain coverage and millimeter-level targeting over portability.
Planned Unnamed Product

Source: Nudge
In April 2025, Nudge stated it was developing a second architecture intended for home and everyday use. Nudge described four workstreams that underpin this direction: shrinking the drive electronics, using more advanced transducer fabrication, embedding an imaging or localization method derived from the MRI-guided approach into the device itself, and enabling per-user personalization of stimulation. No product name has been announced.
The stated ambition is a portable system that could be operated outside clinical settings for disease treatment and, longer term, for cognitive use cases such as focus, sleep, learning, and memory.
Market
Customer
Nudge has not published a customer list, so the profile below can be inferred from the current device’s dependence on MRI and research-grade workflows. The most plausible early adopters are US health systems with MRI capacity and active neuromodulation or imaging research programs, including large academic medical centers and the Veterans Health Administration.
Claims-based utilization data suggest that a large share of MRI procedures flows through high-volume outpatient imaging networks. A 2024 analysis by Definitive Healthcare lists organizations such as American Health Associates, Envision Healthcare, TridentCare, Touchstone Imaging, MedQuest, SDMI, Radiology Associates of North Texas, and Jefferson Radiology among the highest-volume MRI providers, underscoring how much capacity sits outside inpatient settings. This scale is relevant for long-term distribution, but near-term feasibility and early human-use work typically depend on sites that can support non-routine protocols, additional safety screening, and research coordination.
Within those institutions, end users are physicians and clinical researchers in psychiatry, neurology, neurosurgery, and radiology, working with MRI operations. High-throughput outpatient centers prioritize standardized diagnostic slots, whereas research requires dedicated scheduling windows and governance that are more common in academic research units than in retail imaging centers. For example, Beth Israel Deaconess Medical Center’s radiology research program separates research scheduling from routine clinical operations and controls access by project type and funding status. Early engagements should be expected to run under IRB-approved research protocols rather than reimbursed clinical services, with investigators and MRI operations jointly driving adoption at each site.
Market Size
Global neurotechnology spend is projected to grow from roughly $15.3 billion in 2024 to about $52.9 billion by 2034 (13.9% CAGR). Within this category, neuromodulation devices are forecast to reach about $10.7 billion by 2030, up from $6.8 billion in 2025, at a 9.4% CAGR. MRI-guided focused-ultrasound devices remain a smaller, adjacent segment, estimated at $223.5 million in 2024 with 10.1% annual growth to roughly $585.7 million by 2034.
Near-term demand for an MRI-dependent system is concentrated among US health systems and federal facilities that run research-grade imaging workflows. As of 2025, the US had 6.1K hospitals. As of 2022, the AAMC’s Council of Teaching Hospitals and Health Systems comprised approximately 400 teaching hospitals and health systems (this number includes accredited Canadian teaching hospitals), and the VHA operated 171 medical centers nationwide as of 2025.
Availability of MRI is widespread but uneven, and “access” does not necessarily mean on-site ownership. The Neiman Health Policy Institute maintains a state-by-state series on the share of hospitals reporting access to MRI, which can be used to identify states and hospital markets with higher baseline access when prioritizing outreach.
Procedure volume is concentrated among a small number of high-throughput imaging centers, which affects where pilots can run efficiently. In the 2023 dataset, Definitive Healthcare’s claims-based list shows single outpatient centers accounting for 1–7% of all U.S. MRI procedures each, with American Health Associates at 6.7% and several others between ~1.7% and ~2.7%. This concentration suggests a small set of operators could support sizable feasibility work and later inform broader rollouts. Nudge has not disclosed customers, so the addressable market framing above is inferred from the current device’s reliance on MRI suites and research workflows rather than announced buyer lists.
Competition
Competitive Landscape
Clinical options relevant to anxiety and related mood disorders, chronic pain, and substance use fall into four groups: implantable devices (deep-brain stimulation), non-invasive devices (e.g., transcranial magnetic stimulation and other energy-based tools), pharmaceutical interventions (e.g., SSRIs/SNRIs, esketamine, medications for opioid use disorder), and prescription digital therapeutics. These categories define the reference points against which an MRI-guided, non-invasive ultrasound system will be compared.
Buyer comparisons in Nudge’s space will be based on four main factors: the ability to engage deep-brain targets without surgery; the ability to plan and verify dose and target with objective readouts; the day-to-day delivery setting and staffing requirements (outpatient clinic, surgical suite, or MRI room); and the presence of coverage precedent from Medicare or large commercial payers.
Incumbents
Neuromodulation hardware: The FDA first cleared a Transcranial magnetic stimulation (TMS) system for major depressive disorder in 2008, and deep-TMS systems added OCD in 2018 and smoking cessation in 2020. Coverage is broad through Medicare local coverage determinations and commercial policies, which lowers adoption friction for MDD and OCD workflows. It is currently delivered in outpatient clinics. TMS mainly affects the surface cortex; attempts to reach deeper structures trade focus for depth, which constrains target selection compared with deep-brain approaches.
Deep-brain stimulation (DBS): DBS is established in surgery-capable centers. The FDA granted a Humanitarian Device Exemption for DBS in treatment-resistant OCD in 2009, enabling use under IRB oversight at each site. However, it carries the risks of surgery and ongoing device management. DBS provides direct access to deep targets and is supported by large device makers with installed surgical footprints; the surgical pathway and IRB obligations limit the number of eligible centers and patients compared with non-surgical options.
MRI-guided focused ultrasound (ablative): MRI-guided focused ultrasound is approved in the U.S. for lesioning in movement disorders and runs inside an MRI suite. This establishes that MRI-coupled energy delivery can be regulated and reimbursed, but current approvals are for permanent ablation rather than reversible neuromodulation.
Pharmaceuticals: SSRIs and SNRIs are first-line for anxiety and depression, with wide availability and payer coverage. However, individual response and adherence to the pharmaceuticals vary, and adverse effects are common. Esketamine nasal spray (Spravato) received FDA approval for treatment-resistant depression in 2019 and requires in-clinic administration under a REMS program, which raises per-treatment cost and staffing needs but offers a covered non-surgical option. For substance use, medications for opioid use disorder, such as methadone and buprenorphine, reduce mortality in meta-analyses and are the standard of care, though retention and access constraints persist.
Prescription digital therapeutics (PDTs): The FDA authorized the first software-only treatment for substance-use disorder in 2017, and an additional device for PTSD-related nightmares followed in 2020. Reimbursement has been uneven, and Pear Therapeutics, an early category leader, filed for Chapter 11 in 2023. PDTs show that software can achieve treatment claims through FDA pathways; Medicare adoption remains case-by-case, which affects how quickly new categories translate clinical evidence into paid use.
Startups
Neuralink: Neuralink, which was founded in 2016, operates in fully implantable brain–computer interfaces for high-bandwidth neural recording and stimulation. The FDA cleared its first in-human IDE in May 2023, and the first human implant occurred in January 2024 under the PRIME study. In June 2025, Neuralink announced a $650 million Series E at a $9 billion valuation, bringing its total funding to $1.3 billion. Compared to a non-invasive LIFU device like Nudge, Neuralink is invasive and remains investigational in the United States. Capabilities demonstrated by trial participants include thought-based cursor control and typing control, as part of Neuralink’s established mission of “restoring autonomy”.
InSightec: Founded in 1999, InSightec operates MRI-guided focused ultrasound (Exablate Prime) for functional neurosurgery. FDA premarket approval covers essential tremor and tremor in Parkinson’s disease. In July 2025, the FDA cleared staged bilateral treatment for advanced PD. In 2024, the company raised a $150 million funding round that brought its total funding to $882.9 million, led by Koch Disruptive Technologies.
Relative to Nudge, Insightec has established MRI-suite workflows and coverage precedents. As of July 2025, Insightec had treated more than 25K patients with movement disorders across 197 centers globally. However, Insightec performs permanent lesioning rather than reversible neuromodulation. This could be a point of friction for patients should reversible options like Nudge arise. Despite this, Insightec’s capability is incisionless and MRI-guided.
Magnus Medical: Magnus Medical was founded in 2020 and operates non-invasive brain stimulation for psychiatry and commercializes SAINT, an MRI-informed accelerated intermittent theta burst stimulation (iTBS) protocol for major depressive disorder, cleared in 2022. Its US launch was in 2024, and CMS finalized outpatient payments effective January 2025. The company has raised a total of $114.3 million in funding as of June 2026. Magnus is a reimbursed comparator in outpatient reversible neuromodulation entirely focused on treating depression through its protocol.
Openwater: Openwater, founded in 2016, develops a wearable low-intensity focused-ultrasound (LIFU) platform for non-invasive brain modulation. R&D devices were shipped to early adopters for research use for $10K. As of June 2026, the company had raised a total of $76 million in funding. Like Nudge, Openwater is working on non-invasive, reversible LIFU; Openwater is focused on treating cancers, mental illness, strokes, and autoimmune conditions, with eventual ambitions to enable BCI.
Neurosona: Neurosona is a South Korean company founded in 2017 that develops transcranial focused-ultrasound neuromodulation systems for both psychiatric and neurodegenerative conditions. A Korean Alzheimer’s pilot was completed in 2025, and the published work cites Neurosona devices in studies of Major Depressive Disorder and Alzheimer’s Disease. The company is a subsidiary of TS Nextgen, which invested 5 billion KRW (approximately $3.7 million) in the company in May 2024. Like Nudge, Neurosona is a non-invasive LIFU entrant. However, its capability is limited to early human studies and domestic development for MDD, AD, disorders of consciousness (like comatose states), neuropathic pain, sleep disorders, and strokes.
Business Model
Nudge's go-to-market strategy follows a clinical-to-consumer arc. The company plans to first use Nudge Zero to address acute medical conditions, with the longer-term goal of creating a headphone-like miniaturized version to enhance mood, cognition, and daily life for healthy people. Co-founder Quintin Frerichs has described the highest-impact near-term use cases as increasing wellbeing and the ability to think clearly and learn quickly, with particular promise for people struggling with mental health challenges. Nudge has not disclosed pricing or initiated monetization.
Traction
Nudge is running first in-human feasibility work on a larger, non-invasive LIFU system; feasibility at this phase is a limited, small-n clinical investigation used to assess initial clinical safety and basic device functionality, with allowance for design iteration under an Early Feasibility Study (EFS) IDE. Neuromodulation systems of this type are generally treated as significant-risk devices and therefore enrollment proceeds only after both FDA approval of an Investigational Device Exemption (IDE) and Institutional Review Board (IRB) approval.
Following feasibility, the program will need controlled clinical trials designed to demonstrate safety and effectiveness for the intended use, using pre-specified endpoints and appropriate controls (including randomization/sham where feasible) consistent with FDA’s pivotal-study design guidance.
Valuation
In July 2025, Nudge raised a $100 million Series A round at an undisclosed valuation led by Greenoaks and Thrive Capital, which remained its total funding as of June 2026. The company stated it would use the new capital to develop and vertically integrate “hardware, software, and neuroscience”. Nudge plans to achieve this by developing the hardware and algorithms for ultrasound-based brain imaging, hiring domain experts, engineers, and researchers.
Key Opportunities
Consumer Neuromodulation
In the US, prescription device distribution and labeling (21 CFR 801.109) and the FDA’s Home Use guidance together govern design, human factors, and labeling for lay use, so a consumer-facing neuromodulation device that makes treatment claims must comply with these frameworks rather than rely on the general-wellness policy.
This provides a route for prescription at-home neuromodulation in the US regulatory environment. Multiple non-implant devices are cleared for prescription use and labeled for use outside clinical settings, including gammaCore non-invasive vagus nerve stimulation for migraine/cluster headaches, Nerivio remote electrical neuromodulation for migraines, and Cala kIQ for tremor in essential tremor and Parkinson’s disease. These precedents indicate that prescription neuromodulation with home use is viable when indications, labeling, and risk controls are supported by evidence.
Proprietary MRI–FUS dataset
A large, de-identified MRI-plus-ultrasound dataset can be monetized in two possible ways. Once cleared, it can underpin software sold to hospitals: Medicare already pays per-use for several imaging AI/quant tools, including Optellum lung-nodule risk ($650) and 4DMedical ventilation analysis ($650). These precedents suggest that hospitals and payers are already funding image-based software developed on curated datasets.
Second, such datasets can be licensed directly. Major repositories charge access fees (e.g., UK Biobank imaging data), and commercial brokers (e.g., Segmed) aggregate and sell de-identified imaging data, including partnerships with pharmaceutical and technology platforms, and have a reported network now exceeding 100 million studies. Companies are also paying hospitals for de-identified patient data to train AI. These market signals indicate that curated imaging datasets are an established, paid commodity for life sciences R&D and model development.
Defense or Government R&D Collaboration
US defense and advanced research agencies continue to fund non-invasive neurotechnology and brain health programs. While DARPA’s N3 (Next-Generation Nonsurgical Neurotechnology) program is complete, newer efforts include ARPA-H’s FRONT program (Functional Repair of Neocortical Tissue), launched in July 2025. Meanwhile, the DoD’s Warfighter Brain Health Initiative highlights sustained interest in brain-health monitoring and interventions.
Key Risks
Unproven Regulatory Path
Focused ultrasound approvals in neurology are for irreversible thermal ablation (e.g., Insightec), but not for reversible ultrasound neuromodulation. Reviews in 2024 and 2025 continue to describe transcranial focused ultrasound (tFUS)/transcranial ultrasound stimulation (TUS) neuromodulation as investigational without FDA marketing authorization. If the device is deemed a significant-risk device, US studies may only begin after both FDA investigational device exemption approval and IRB approval.
Adoption and Workflow Constraints
MRI-guided workflows require access to compatible scanners, trained staff, and site readiness. However, Medicare policies for procedure coverage have historically followed FDA approvals on a condition-by-condition basis. These dynamics can potentially slow early deployment and limit initial site count until clinical and economic evidence grows.
IP Defensibility Risk
Openwater’s “Open Source, Always” stance (AGPL/CC-BY-SA plus a patent pledge) and public RUO documentation reduce information barriers for ultrasound neuromodulation, increasing the likelihood of imitation or parallel development. Nudge’s defensibility may begin to rely more on clinical evidence, regulatory assets, and integrations than on intellectual property around hardware.
Summary
Anxiety, chronic pain, and addiction affect large U.S. populations with multi-hundred-billion-dollar annual costs and meaningful treatment resistance, creating room for alternatives to drugs and surgery. Nudge is developing a non-invasive, MRI-verified focused-ultrasound system to modulate deep brain circuits and is running early human feasibility studies in San Francisco. The company raised $100 million in Series A funding in July 2025 to fund device engineering, MRI-based targeting tools, and supporting software. In a landscape that includes outpatient TMS (cleared and reimbursed for depression/OCD), MRI-guided focused ultrasound for ablative procedures (Insightec), and modular LIFU kits (Openwater), Nudge’s approach targets reversible neuromodulation with MRI planning and verification inside the scanner. Regulatory and payment tailwinds (FDA’s Breakthrough Devices Program and CMS’s TCET pathway) decrease the traditional distance between clinical signal and Medicare coverage, while public-sector brain programs (e.g., DARPA/ARPA-H) indicate ongoing non-dilutive funding channels. Beyond the scanner-based system, Nudge discloses a second, portable architecture in development for consumer use. Overall, the company is moving from initial feasibility toward a platform that combines imaging-guided neuromodulation, workflow software, and a potential home-use line, with near-term customers expected to be MRI-capable research hospitals and federal sites before broader distribution.

